Burnout is very important to nurses’ physical and mental health and career development. Current approaches to assessing nurse burnout tend to use a total score modeling paradigm to explore the impact of external factors on burnout. The purpose of this study is to delve into the item-level relationship between nurse burnout and its influencing factors at both the social and psychological levels using a network analysis approach.
This study was conducted in June 2023 and 1,005 nurses from 4 hospitals out of 8 tertiary care hospitals in Harbin were selected to participate in this study using whole cluster sampling method. Measurements included a general demographic questionnaire, Trait coping styles questionnaire, Organizational commitment questionnaire, Work-family conflict scale, Transformational leadership questionnaire, and Maslach Burnout Inventory-General Survey.
Our results suggest that “C1 Time-Based work interference with family” showed the strongest centrality and bridging in the overall network. This finding underscores its centrality to burnout. Other strongest bridge symptoms included “E2 Reduced personal accomplishment” and “A1 Positive coping styles” indicating their strongest connections to other clusters.
Nurse administrators should be encouraged to pay more attention to nurses’ work situations and family distress, and to help nurses in a flexible way.
Nurses are facing global concern as a high-risk group for burnout [1]. Burnout was first introduced in 1974 as physiological and psychological exhaustion resulting due to unrelieved chronic job stress [2]. Burnout is a negative emotional experience that not only affects nurses’ physical and mental health and work efficiency, but also reduces the morale and service quality of the nursing team [3]. In turn, it affects patient satisfaction [4], leading to consequences such as strained doctor-patient relationships and escalating medical malpractice claims [5]. Nowadays, due to the changing disease spectrum and the aging population, there is an increasing need and demand for quality of care environment and services. There is no doubt, the dramatic increasing work pressure and challenges, lead them more vulnerable to suffer from burnout. Surveys in different countries have shown that 78% of Swedish nurses and 34% of American nurses sufferred from burnout [6], and 10% of nurses in Brazil’s top hospitals experience burnout, while 55% are predisposed to it [7]. In comparison, the incidence of burnout among nurses in China is currently at a high level, with 59.1-69.1% [8]. The high incidence and serious adverse consequences of nurse burnout lead it to be paid more and more attention.
The three-dimensional theoretical model of job burnout posits that job burnout comprises three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment [9]. These dimensions are both independent and interconnected, and individuals may experience varying levels of job burnout across different projects [10]. While previous studies have identified numerous factors influencing nurses’ burnout, complex correlations among these factors exist. The current literature has not fully elucidated their independent contributions or whether they interact with each other or jointly act on potential mediating/regulating mechanisms in the formation process of burnout. Specifically, identifying which factor plays a leading role remains a gap in this research field. Additionally, there may be unrecognized confounding variables in the effect transmission path. Consequently, some studies have proposed intervention strategies to alleviate nurses’ job burnout; however, due to the ambiguity surrounding the underlying mechanism, the actual effectiveness of these measures is often limited. Therefore, further exploration into the nature and multidimensional complexity of nurses’ job burnout through network analysis can address this gap. Firstly, this method can more carefully depict the multi-dimensional characteristics of nurse burnout to provide a comprehensive understanding of its essence. Secondly, by conducting an in-depth analysis of the internal connections and interactions between various dimensions and influencing factors using network analysis methods can reveal the complex causes and dynamic change processes associated with job burnout. This approach can help identify key driving factors for job burnout as well as meaningful connections between various dimensions to facilitate targeted solutions for addressing this issue.
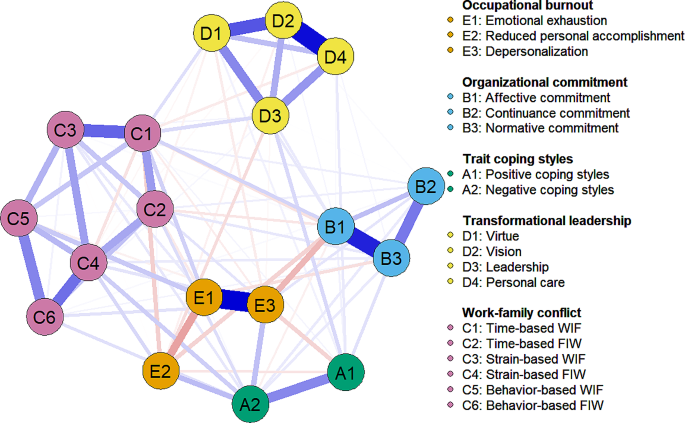
Network analysis, as a tool for mathematical analysis and visualization of relationships between complex variables, is particularly suitable for dealing with the topic of this study [11]. Compared to more traditional ways of presenting variable relationships, network diagrams allow the intrinsic associations and interactions between variables to be presented in a more intuitive, clear and unambiguous way. Because the core concepts of network analysis include “nodes” and “edges”, which together form a network graph, edges connect these nodes, demonstrating the direct or indirect dependencies and connections between them [12]. The most commonly used approach to network analysis is based on regularization and estimation of partial correlations between all pairs of symptoms, i.e., edges in the network represent unique pairwise relationships between two nodes [13]. In contrast to traditional latent variable models and simple correlation methods, network analysis not only provides a centrality index for each node, quantifying its importance in the network, but also identifies “central symptoms” that may trigger other symptoms, i.e., the variable that has the greatest impact on the network as a whole. In addition, network analysis can identify “bridge symptoms” that serve as transitions between syndromes [14, 15], i.e., key variables that mediate transitions between different variables. Therefore, the networked presentation not only greatly deepens our understanding of the complex intertwined relationships between variables, but also provides a powerful tool and foundation for subsequent in-depth scientific analyses and the design of targeted intervention strategies. Locating the central symptom in the network through network analysis provides a more precise and efficient entry point for psychosocial interventions for nurse burnout [16].
For a more comprehensive understanding of nurses’ burnout, we draw on the triadic reciprocal determinism proposed by psychologist Bandura (1989) [17]. The theory emphasizes the inalienable interplay between internal and external factors. Bandura believes that individual behavior is the result of the interaction between the behavior itself, the internal state of the individual and the external environment [18]. Specifically, individual behavior is not only driven by internal psychological states (such as cognition, emotion, and motivation), but also deeply shaped by external environments (such as social culture, organizational climate, etc.). From this theoretical perspective, nurse burnout is a multi-dimensional and complex phenomenon, and its cause cannot be explained by a single factor. The social level involves factors such as working environment, organizational culture, interpersonal relationship and career support, while the psychological level includes individual psychological state, coping mechanism, emotional management and career identity. There is a close interaction between these two levels, which jointly affect the level of nurses’ burnout. Reviewing the previous studies, most of them focused on an in-depth discussion of a certain aspect of job burnout, lacking a cross-level and multi-dimensional comprehensive analysis [19]. Therefore, this study chooses to start from both social and psychological aspects and adopts network analysis method to reveal a comprehensive discussion on the causes of nurses’ job burnout, so as to provide scientific basis for formulating more comprehensive and effective intervention measures, so as to effectively reduce nurses’ job burnout.
The social dimension focuses on two factors, work-family conflict and transformational leadership, both of which have a profound and multidimensional impact on nurses’ professional experience as typified by the external environment of the workplace and leadership style. Role theory states that people play different roles in different domains, and these roles have different expectations and demands on the individuals [20]. The work-family conflict proposed by Greenhaus [21] is a type of inter-role conflict, which, if not properly resolved, may lead to increased burnout [22, 23]. That is to say, nurses who are able to better balance their work and family roles and reduce this conflict may reduce the risk of burnout [24]. In addition, while focusing on work-family conflict, leadership styles in organizations also need increased attention. Transformational leadership style in organizations can be an important factor in mitigating burnout [25,26,27,28]. This leadership style can make employees realize the importance of tasks, stimulate their internal motivation, and then push them to exceed expectations, thus reducing the possibility of burnout [29]. At the psychological level, the two factors chosen were and organizational commitment and coping styles, which are closely related to the construction of nurses’ professional identity and the individual’s psychological adjustment process, and together constitute an indispensable part of nurses’ daily work and life, and have a significant moderating effect on the level of nurses’ burnout. Coping style is the factor that has a significant relationship with burnout [30,31,32,33,34]. Coping is a cognitive and behavioral strategy adopted by individuals when facing stressful situations [35, 36]. Positive coping styles can significantly reduce emotional exhaustion, thereby decreasing the risk of burnout [37], whereas negative coping styles may exacerbate burnout. In addition, organizational commitment is an important factor influencing individuals’ psychological attitudes and behavioral choices. Organizational commitment refers to the degree to which an individual identifies with and is committed to an organization [38]. Increasing the level of organizational commitment among nurses can help reduce the risk of burnout [39]. A strong organizational commitment can save those who are closely connected to the organization from burnout. Therefore, to be specific, the four influences of work-family conflict, transformational leadership, trait coping styles, and organizational commitment were included in this study’s network to explore their association with nurse burnout.
In summary, this study aims to deeply explore the item-level relationship between nurse burnout and its influencing factors from both social and psychological levels based on the network analysis method and according to the triadic reciprocal determinism. Specifically, we will reveal the deep mechanism of burnout by analyzing the centrality of these components to burnout symptoms and the complex relationship between them. This study is expected to provide targeted intervention references for managers in healthcare organizations, as well as guidance for nurses’ career development and improve the status quo of nurses’ burnout. It would be a great significance in maintaining the stability and sustainable development of the nursing workforce.
Triadic Reciprocal Determinism (TRD) is a conceptual framework in social cognitive theory, which was introduced in 1971, and focuses on the dynamic interaction between personal factors (e.g., intrinsic drives such as cognition and emotion), environmental factors (e.g., external conditions such as the physical environment, family, and friends), and individual behaviour. The theory is based on the following principles. First, the theory emphasises the causal interaction between individuals and behaviours. Individuals and behaviours interact; individual perceptions can stimulate and maintain behaviours, and behaviours can be influenced by the level of individual perceptions. Second, there is a causal interaction between behaviour and environment. Behaviour and environment influence each other. The environment nurtures behaviour and promotes it. Third, the causal interaction between the environment and the individual. The environment and the individual influence each other.
Person-environment fit model (P-E): It was proposed by Malles and Leiter, who believed that burnout is not purely a matter of individual stress, but is the result of the interaction between the individual and the environment, and that the mismatch between the individual and the organization produces job burnout. The theory emphasizes that not only do individual and environmental variables directly influence individual behaviour, but the interaction between the individual and the environment in which they are placed is an important influence on individual behaviour. Therefore, this study is based on this model to explain burnout in terms of matching between individual and environmental aspects.
In this study, the triadic reciprocal determinism is used as the basis and the person-environment fit model is used as a secondary theoretical basis to analyze the complex relationship between the individual (especially organizational commitment and coping styles), the behaviour (which is specifically manifested in the phenomenon of burnout), and the environment (focusing on the dimensions of work-family conflict and transformational leadership). It helps us to analyze in depth the interrelationships and mechanisms of influence between these elements.
This study was conducted in June 2023 and 1,005 nurses from four hospitals out of eight tertiary care hospitals in Harbin were selected to participate in this study using whole cluster sampling method (see Table 1 for general information). The study used strict inclusion criteria, specifically targeting nurses who had practiced as registered nurses for at least six months. Nurses whose primary duties were not directly involved in patient care (e.g., nurses in the central sterile supply department) and practicing nurses were excluded from the study. In designing and distributing the questionnaire, we took into full consideration the nurses’ day shift, night shift, weekend and holiday duty. In particular, we extended the time for completing the questionnaire to one week so that nurses could complete the questionnaire at a suitable time according to their work schedule. In addition, this investigation was formally approved by XXX to ensure the integrity and ethical validity of the study. All participants completed the questionnaire after signing the written informed consent to ensure accuracy and strict confidentiality. Data were imported using SPSS software and data were analyzed using R software.
Demographic information collected includes gender, administrative office, marital status, education level.
The work-family conflict scale compiled by Carlson [40] was adopted. The scale has six dimensions, the six dimensions of conflict measured include the combination of three forms of work-family conflict (time, strain, and behavior) and two directions of work-family conflict (work interference with family and family interference with work). When these three forms and two directions are combined six dimensions of work-family conflict result: (1) time-based WIF, (2) time-based FIW, (3) strain-based WIF, (4) strain-based FIW, (5) behavior-based WIF, and (6) behavior-based FIW, Use the Likert 5-point score, which indicates the level of conflict. The scale has good reliability and validity in nurse studies, with a Cronbach’s alpha coefficient of 0.899 in this study.
Based on Bass’s multifactor leadership questionnaire [41], Transformational Leadership Questionnaire (TLQ) was modified and translated in Chinese by Li CP with a good content reliability [42, 43]. The TLQ scale includes 26 items and 4 dimensions: virtue, leadership, vision, and personal care. Each item was answered by using a Likert 5-point scale (1 = strongly disagree; 5 = strongly agree). A higher score of TLQ indicates a higher level of transformational leadership that the respondents perceived from their leaders are. In this study the total questionnaire Cronbach’s alpha coefficient was 0.982, of which the Cronbach’s alpha coefficient for virtue was 0.961, the Cronbach’s alpha coefficient for vision was 0.949, the Cronbach’s alpha coefficient for personal care was 0.952 and the Cronbach’s alpha coefficient for leadership was 0.941.
Coping styles were assessed and measured using the Trait Coping Styles Questionnaire (TCSQ). The questionnaire contains two main factors: negative coping (NC) and positive coping (PC), each of which contains 10 entries. Each entry was scored on a Likert 5-point scale, where 1 means “definitely not” and 5 means “definitely yes”. It is worth mentioning that the reliability and validity of the TCSQ have been fully validated [44]. In this study the total questionnaire Cronbach’s alpha coefficient was 0.862, of which the Cronbach’s alpha coefficient for positive coping was 0.822 and the Cronbach’s alpha coefficient for negative coping was 0.849.
Organizational commitment was assessed using the Organizational Commitment Questionnaire (OCQ), which covers three dimensions of affective commitment, continuance commitment and normative commitment, with a total of 18 entries [45]. The scale was scored on a Likert 5-point scale, where 1 represents “strongly disagree” and 5 represents “strongly agree”. The higher the score, the higher the level of organizational commitment. The scale has good reliability and validity in nurse studies. In this study the total questionnaire Cronbach’s alpha coefficient was 0.907, of which the Cronbach’s alpha coefficient for affective commitment was 0.890, the Cronbach’s alpha coefficient for sustained commitment was 0.833 and the Cronbach’s alpha coefficient for normative commitment was 0.747.
For the assessment of burnout, we used the domestic MBI-GS scale revised in 2002 by Professor Li Chaoping of the School of Public Administration of Chinese University [46]. The scale consists of 15 entries including three dimensions of emotional exhaustion, depersonalization and reduced personal accomplishment. A Likert 7-point scale was used. Emotional exhaustion and depersonalization dimensions were scored positively, the higher the score, the more serious the burnout; reduced personal accomplishment dimensions were scored negatively, the higher the score, the less severe the burnout. The Chinese version of the MBI-GS has been widely used in the Chinese population and has demonstrated good reliability and validity. In this study the total questionnaire Cronbach’s alpha coefficient was 0.875, of which the Cronbach’s alpha coefficient for emotional exhaustion was 0.762, the Cronbach’s alpha coefficient for depersonalization was 0.918 and the Cronbach’s alpha coefficient for personal accomplishment was 0.816.
To evaluate and visualize the network, the R-packages “qgraph” [12] and “bootnet” [47] Tools were utilized. The network structure was estimated using the enhanced least absolute shrinkage and selection operator (eLASSO) method, which combines logistic regression analysis with an optimization process to determine the optimal connection method for each symptom. The algorithm yields a sparse network model that is more interpretable than the original model. Model selection is based on the Extended Bayesian Information Criterion (EBIC) [48, 49].
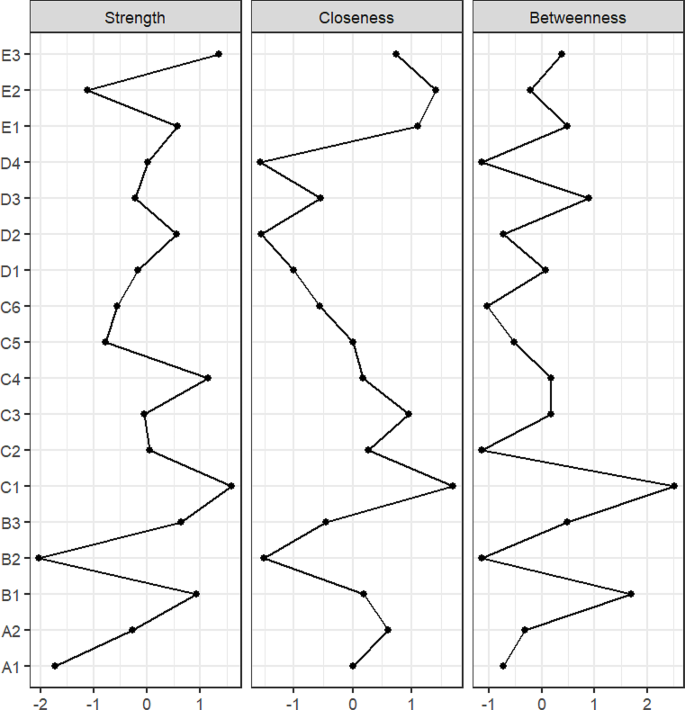
The centrality indices (including strength, closeness and betweenness) was estimated using the centrality graph function of the “qgraph” package to study the strength of each node and determine which symptoms are most important in the network [50]. Node strength reflects the degree to which a node is directly connected to the network. Closeness, on the other hand, measures the degree to which nodes are indirectly connected to the network. Betweenness focuses on the degree to which nodes are indirectly connected to the network. In this analysis, the importance of strength centrality was particularly emphasized because it is proportional to the degree to which a given node uniquely explains the variance of the nodes to which it is connected, and is a better indicator of the strength of network centrality [51]. The centrality index was standardized to a z-score. In addition, in order to identify key pathways between burnout symptoms and various environments, a bridge analysis was conducted to identify influential bridge nodes. Bridge nodes are viewed as nodes that potentially act as links between broader communities of nodes [52]. The “bridge” function in the “networktools” package is utilized to calculate bridge strength and identify potential bridge nodes.
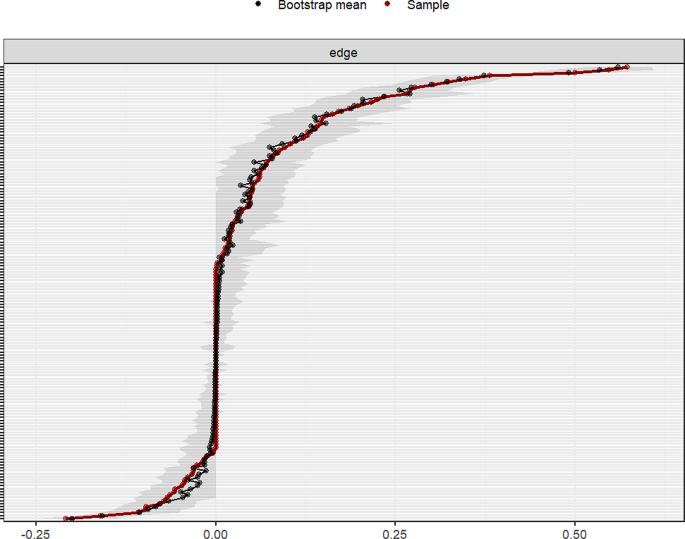
The accuracy and stability of the network model was assessed by using the R-package “bootnet” [47]. First, confidence intervals (CIs) were calculated using a nonparametric bootstrap method to assess the accuracy of the edge weights [53]. Next, a new dataset was created by randomly resampling the observations in the dataset and computed 95% CIs from it. A larger CI indicates a lower accuracy of the edge estimation, while a narrower CI indicates a higher confidence in the network [47]. In this network analysis, 1000 permutations have been performed and bootstrap differential test was used to assess the differences in network attributes. To quantify the stability of the metrics, the correlation stability coefficient (CS coefficient) was calculated [54]. The CS coefficient indicates the maximum proportion of samples that can be deleted with a correlation with the original centrality metrics of at least 0.70. Generally, the CS coefficient should not be less than 0.25 and ideally should be higher than 0.50 [41].
In the present study, a total of 1005 participants met the study inclusion criteria, including 261 males and 744 females. The basic socio-demographic characteristics of the participants are detailed in Table 1 below, while the symptom data measured by the scales, including mean, standard deviation (SD), skewness, and kurtosis, have been organized in Table 2.
The centrality index is used to assess the overall importance of the symptom in the network of events and symptoms (Opsahl, Agneessens, & Skvoretz, 2010). From Fig. 2 we can find. In terms of the strength of the centrality index, “C1 Time-based WIF”, “E3 Depersonalization”, and “C4 Strain-based FIW” show the strongest strength and are the central symptoms in this network. In terms of closeness, the three burnout symptoms had the highest levels of intimacy, while the four dimensions of transformational leadership were relatively low. In terms of betweenness, “C1 Time-based WIF” scored the highest, suggesting that this node may act as a bridge for transferring influences between symptoms and/or environments within the network.
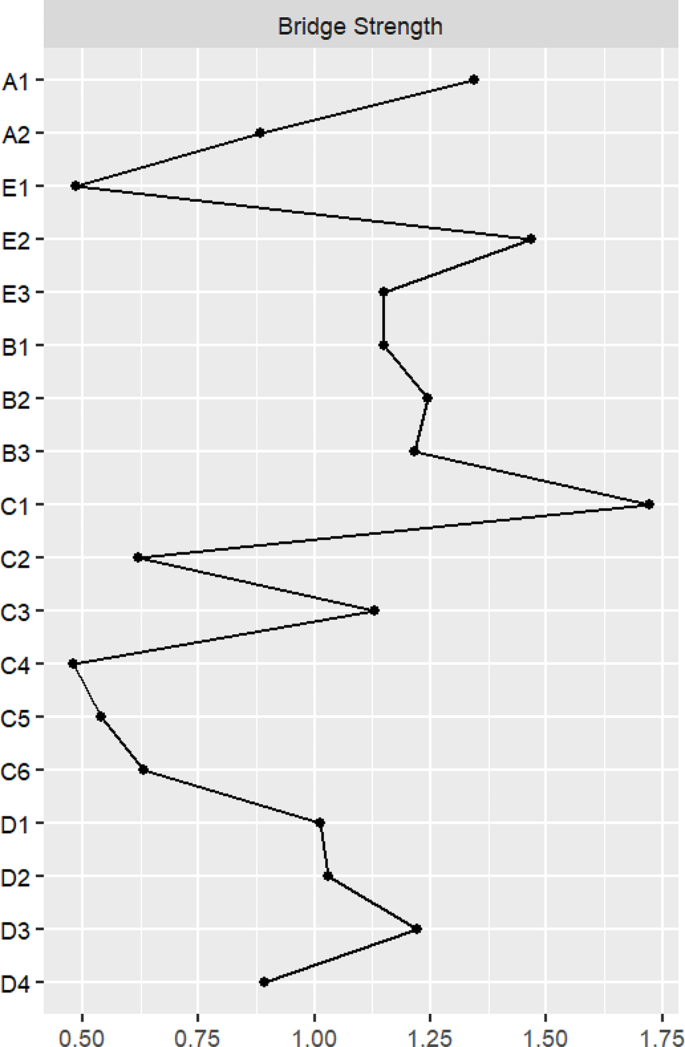
From Fig. 3, we can clearly find that “C1 Time-based WIF”, “E2 Reduced personal accomplishment”, and “A1 Positive coping styles” are the main bridge symptoms connecting different communities. These symptoms not only have a significant impact in their respective dimensions, but also play a crucial role in facilitating communication and cooperation among different clusters.
We use the case-drop bootstrap method to compute 95% confidence intervals for the edge weights. Observations show (e.g., Fig. 4) that these confidence intervals are narrow and mostly overlapping, indicating that our estimates of edge weights in the network have a fairly high accuracy. At the same time, the weights of many edges differ significantly from each other, indicating some heterogeneity in the network. Node strengths can reflect the network structure more stably. The CS coefficient of the strength in the sample is 0.594, which shows that the network structure is more stable.
To the best of our knowledge, this study is the first network analysis of burnout symptoms and their psychological and social influences in a group of Chinese nurses. We found that the correlations between symptoms in the clusters of nurse burnout (E1, E2, E3) were not highly interrelated. “E1 Emotional exhaustion” was positively correlated with “E3 Depersonalization” (weight = 0.57), which is consistent with Wu [55]. The marginal weight between “Emotional exhaustion” and “Depersonalization” was 0.65, and the higher the level of emotional exhaustion, the higher the level of depersonalization [30]. Nurses not only need strong willpower and a positive attitude to cope with the heavy workload, but also need constantly pay attention to the psychological and physiological changes of patients. In the long term, this can lead to depletion of emotional resources and apathy towards others if not properly adjusted. Interestingly, “E1 Emotional exhaustion” was negatively correlated with “E2 Reduced personal accomplishment” (weight=-0.21). On the other hand, “E3 Depersonalization” was not directly associated with “E2 Reduced personal accomplishment” in the network structure of this study. This is different from previous network study conducted in a sample of nurses (where depersonalization was positively associated with reduced personal accomplishment) [55]. The divergence can be attributed to this study’s comprehensive analytical approach that extends beyond examining only the internal dynamics within the three core dimensions of burnout. It encompasses a wide array of multidimensional influencing factors. The intricate interplay among these diverse elements could potentially serve as an intermediary or regulatory mechanism impacting the correlation between ‘E3 Depersonalization’ and ‘E2 Reduced personal accomplishment’. Hence, it is plausible that indirect associations identified in this research stem from mediating or moderating influences exerted by variables beyond those directly related to burnout. This discovery underscores both complexity and multidimensionality inherent in nurse burnout phenomena, offering significant theoretical insights and practical implications for gaining profound insight into its underlying mechanisms while devising more precise interventions aimed at alleviating nurse burnout.
In our network model, the nodes “C1 Time-based WIF”, “E3 Depersonalization”, and “C4 Strain-based FIW” are three key center symptoms. This means that these three nodes play a crucial role in activating and maintaining the entire network. Among the clusters of work-family conflict, “C1 Time-based FIW” is the one we need to focus on most. Time is a key factor that increases nurses’ conflict [56]. Several studies have shown that excessive work hours and work schedules that include weekends reduce nurses’ time at home, which in turn creates work-family conflict [57, 58]. Obviously, work-family conflict is one of the effective predictors of burnout [59]. Past studies have confirmed the negative correlation between time-based work-family conflict and burnout [60], consistent with this study. When workloads accumulate, people attempt to find solutions to complete tasks which would active pursuit tends to enhance personal fulfillment. In addition, “C4 Strain-based FIW” also deserves our attention. Burnout is a long-term response to chronic stress [61]. Since most nurses are female and married, they tend to take on more family responsibilities, such as breastfeeding their children, participating in family activities, and maintaining family relationships, all of which can cause them more stress. In this study, “C4 Strain-based FIW” was positively associated with depersonalization and reduced personal accomplishment in burnout, which is consistent with the findings of Chen [23]. This stress in the family can be reflected in nurses’ work, such as making it difficult for them to concentrate on their work, decreasing quality of work and negative work attitudes, even can lead to burnout. In the burnout cluster, it is important to focus on “E3 Depersonalization”, which is the core symptom of burnout in this network structure, the results of this paper are consistent with the findings of Wu [55] that the higher the degree of depersonalization, the higher the degree of emotional exhaustion [30]. Due to the lack of real understanding of the profession, nurses have low enthusiasm for work and indifferent attitude. This kind of apathy makes it difficult for nurses to regulate emotions. Undoubtedly, they are prone to emotional exhaustion when their mood fluctuates or lasts for a long time.
Bridge strength better reflects cluster relationships [62]. Among all the bridge symptoms, “C1 Time-based WIF”,“E2 Reduced personal accomplishment” and “A1 Positive coping styles” had the strongest bridge strengths. These nodes occupy a core position in the construction of the key connection network between burnout symptoms and their potential influencing factors. They are not only the key path to understand the mechanism of nurse burnout, but also the main target to formulate effective intervention strategies to reduce nurse burnout. Based on the findings, in order to effectively alleviate nurses’ burnout, we can start from the following aspects: firstly, from the perspective of work-family conflict, nurses could communicate with their supervisors or managers to clarify the priorities and time requirements of their work, to avoid dealing with work affairs during non-working hours and to ensure sufficient rest time. In addition, relaxation and stress-reducing exercises, such as meditation and yoga, could be carried out to provide adequate relaxation or rest for the body and mind. Moreover, there is a need to focus on depersonalization of nurses. At last, nurses need to enhance the sense of work identity and fulfillment through enhancing awareness of the importance and significance of nursing work [61].
This study has far-reaching implications for nurse managers as well. First, for the imbalance between work and family faced by nurses, nursing managers should provide professional psychological support and counseling. This can not only help nurses adjust their mindset, but also improve their ability to cope with stress. In addition, nurse managers can improve nurses’ sense of professional identity through performance management and reward mechanisms. Help nurses realize the significance and value of their work so as to stimulate their enthusiasm and commitment to their work. Furthermore, encouraging team building activities and establishing a favorable working atmosphere are also key. Improving mutual understanding and trust through team activities can help relieve work pressure and enhance the cohesion of the nursing team.
The current study has some limitations. First, our study is mainly based on a self-report questionnaire, which leads to a certain degree of subjectivity in the results. Second, because this study was cross-sectional, it was not possible to determine the direction of the relationship between the nodes in the network, and thus the causal relationship between the nodes could not be clarified. In order to gain a deeper understanding of the dynamic relationships between nodes, future studies could use time series data to explore the temporal causal relationships between nodes. In addition, the network structure is limited by the range of nodes studied and there may be factors not included in this study. Other factors such as workplace spirituality and job rumination could be considered in the future.
In this study, an in-depth analysis of the impact of psychological and social factors on nurse burnout was analyzed through a network analysis. “C1 Time-based WIF” showed the strongest centrality and bridging in the overall network. This finding highlights the important influence of work-family conflict as a factor in nurse burnout. At the same time, we also found other core symptoms with strong impacts, which have great potential for development in the prevention and management of burnout in the nurse population. Health care professionals and nurse administrators should be encouraged to pay more attention to nurses’ work situations and family distress, and to adopt a flexible approach to assisting nurses.
The datasets analyzed in this article are not publicly available. Requests to access the datasets should be directed to the corresponding author.
We are grateful to the nurses who generously contributed their invaluable time to participate in this study.